홈 > 연구소 > 논문 / 학술활동
연구소
마마파파&베이비의 핵심인 베이비 드림 난임 연구소는
그간의 연구학술 성과에 안주하지 않고,
늘 한계를 뛰어넘기 위해 노력합니다.
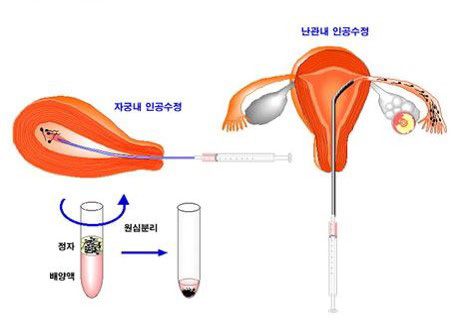
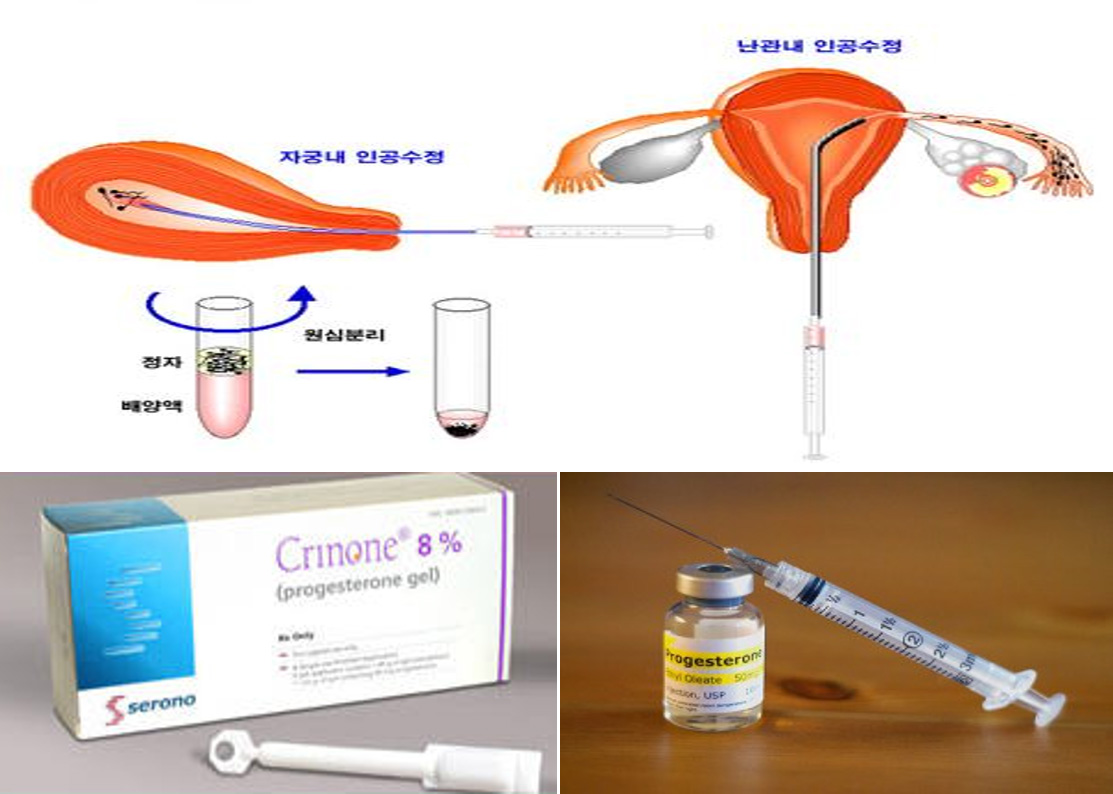
시험관 시술에서 황체기 보강을 위해 질내 프로게스테론 젤에 추가로 저용량의 hCG를 투여하는 것의 효과

2013년 유럽불임학회(ESHRE) P-495 The effect of additional low dose hCG with vaginal progesterone gel in luteal phase of IVF cycles. (시험관 시술에서 황체기 보강을 위해 질내 프로게스테론 젤에 추가로 저용량의 hCG를 투여하는 것의 효과)
I.H. Park1, K.H. Lee1, H.G. Sun1, S.G. Kim1, J.H. Lee1, Y.Y. Kim1, S.A. Kim1, J.D. Cho2.
1 Mamapapa&baby Obstetrics Gynecology Clinic, Obstetrics and Gynecology, Ulsan city, Korea South.
2 Ellemedi Ob&GY, Obstetrics and Gynecology, Changwon, Korea South.
Study question
Does additional low dose hCG supplementation with vaginal progesterone gel is equally effective with intramuscular progesterone as luteal phase support of COH IVF cycles?
Summary answer
In COH IVF cycles, additional low dose hCG supplementation with vaginal progesterone gel makes similar pregnancy rate with intramuscular progesterone as luteal phase support.
What is known already
In a past meta-analyses, clinical pregnancy and delivery rates were significantly improved with intramuscular (IM) progesterone as compared with vaginal progesterone. On the other hand, in some recent RCTs and meta-analyses provided some evidence that no difference existed regarding the clinical pregnancy rate between vaginal progesterone and IM progesterone for LPS. However, many clinicians still prefer IM progesterone to vaginal progesterone due to concern of decreased pregnancy rate with vaginal progesterone.
Study design, size, duration
This retrospective cohort study included 543 women undergoing IVF between January 2011 and December 2012.
Participants/materials, setting, methods
We retrospectively reviewed 543 patients undergoing IVF using GnRH agonist and antagonist protocols. After COH and oocyte aspiration, women received IM progesterone only (Group A) or vaginal progesterone with additional low dose hCG three times (Group B) (1000 IU, OPU day, ET day, ET+3 day).
Main results and the role of chance
349 patient received IM progesterone only as LPS and vaginal progesterone with low dose hCG was given to 194 women. In each group, age (35.9±4.28 vs. 35.06±4.37), endometrial thickness (10.39±2.11 vs. 10.33±2.13), number of transferred embryos (2.0 vs2.0) and percentage of top quality embryo (60.7% vs. 59.3%) did not show significant difference. There were no significant differences between two groups in the pregnancy rate [52.7%(184/349) vs. 49.0%(95/194), P=0.2], spontaneous abortion rate[9.8%(18/184) vs. 8.4%(8/95), P=0.3], ongoing pregnancy rate [47.6%(166/349) vs. 44.8%(87/194), P=0.14].
Limitations, reasons for caution
This is a retrospective study. A prospective randomized study would have minimized potential limitations. And we don’t have comparison group using vaginal progesterone only as LPS due to previous experience of decreased pregnancy rate with vaginal progesterone only [PR 35.7%(5/14)].
Wider implications of the findings
The intravaginal route of progesterone supplementation in IVF has gained wide application as a first choice luteal support regimen, mainly due to comfort and effectiveness of patient. In spite of some RCTs and meta-analyses proving efficacy of vaginal progesterone, many clinicians have met episode of vaginal bleeding before pregnancy test and some have experienced decreased pregnancy rate. With additional low dose hCG, vaginal progesterone could be more secure LPS and really equivalent to IM progesterone.
Study funding/competing interest(s)
Funding by hospital/clinic(s)
Mamapapa&baby Obstetrics & Gynecology clinic
-
 2016년 유럽불임학회(ESHRE) P-062
인공수정시술을 하기 전 얼마나 오래 금욕을 해야 하는가?
2016년 유럽불임학회(ESHRE) P-062
인공수정시술을 하기 전 얼마나 오래 금욕을 해야 하는가?
-
 2015년 미국불임학회(ASRM) P-344
과배란 인공수정에서 매일 황체기 보강을 하는 것이 임신율 향상에 도움을 준다.
2015년 미국불임학회(ASRM) P-344
과배란 인공수정에서 매일 황체기 보강을 하는 것이 임신율 향상에 도움을 준다.
-
 2015년 미국불임학회(ASRM) P-267
자연주기에서 단순화한 검사에 의한 동결란 이식은 체외수정시술결과에 영향을 주지 않는다.
2015년 미국불임학회(ASRM) P-267
자연주기에서 단순화한 검사에 의한 동결란 이식은 체외수정시술결과에 영향을 주지 않는다.
-
 2015년 유럽불임학회(ESHRE) P-769
일측 난관수종이 있는 경우, 거의 절반의 경우 반대쪽 난관에 이상이 있어 추가적인 수술이 필요하다.
2015년 유럽불임학회(ESHRE) P-769
일측 난관수종이 있는 경우, 거의 절반의 경우 반대쪽 난관에 이상이 있어 추가적인 수술이 필요하다.
-
 2014년 미국불임학회(ASRM) P-822
경미한 희소정자증을 보일 때 미세수정을 통한 시험관 시술이 반드시 필요한가?
2014년 미국불임학회(ASRM) P-822
경미한 희소정자증을 보일 때 미세수정을 통한 시험관 시술이 반드시 필요한가?
-
 2014년 유럽불임학회(ESHRE) P-045
반복 유산 여성에서 미세수정을 통한 시험관 시술은 자연 유산을 감소시키지 않는다.
2014년 유럽불임학회(ESHRE) P-045
반복 유산 여성에서 미세수정을 통한 시험관 시술은 자연 유산을 감소시키지 않는다.
-
 2014년 유럽불임학회(ESHRE) P-506
과배란시험관 시술 시에 hCG 주사일에 FSH 투여하는 것이 미치는 영향
2014년 유럽불임학회(ESHRE) P-506
과배란시험관 시술 시에 hCG 주사일에 FSH 투여하는 것이 미치는 영향
-
 2013년 유럽불임학회(ESHRE) P-495
시험관 시술에서 황체기 보강을 위해 질내 프로게스테론 젤에 추가로 저용량의 hCG를 투여하는 것의 효과
2013년 유럽불임학회(ESHRE) P-495
시험관 시술에서 황체기 보강을 위해 질내 프로게스테론 젤에 추가로 저용량의 hCG를 투여하는 것의 효과
울산광역시 남구 삼산로 247 마마파파앤베이비 빌딩 15F - 17F
TEL 052-258-6006 / FAX 052-258-6026
Copyright © mamapapa&baby All Rights Reserved.