홈 > 연구소 > 논문 / 학술활동
연구소
마마파파&베이비의 핵심인 베이비 드림 난임 연구소는
그간의 연구학술 성과에 안주하지 않고,
늘 한계를 뛰어넘기 위해 노력합니다.
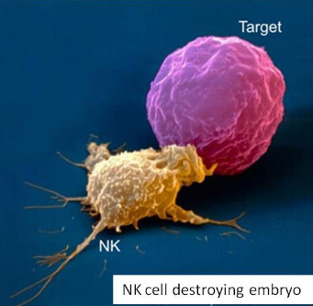
반복착상 실패 환자 에서 면역치료요법이 유용할 것인가; 특히 높은 자연살해세포를 가진 환자에서?
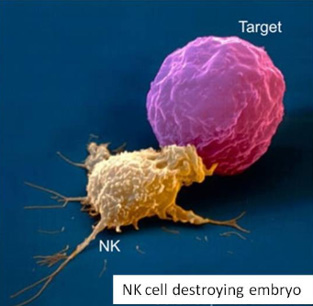
2016년 미국불임학회(ASRM) P-595 IS IMMUNOTHERAPY USEFUL IN RECURRENT IMPLANTATION FAILURE PATIENTS; ESPECIALLY WITH HIGH NATURAL KILLER CELL? (반복착상 실패 환자 에서 면역치료요법이 유용할 것인가; 특히 높은 자연살해세포를 가진 환자에서?)
H. Sun,1 K. Lee,1 I. Park,1 S. Kim,1 H. Chi,1 J. Kim,1 J. Cho2; 1Mamapapa & Baby OB&GY Clinic, Ulsan,
Korea, Republic of, 2Ellemedi Women's Hospital, Changwon, Korea, Republic of
OBJECTIVE
IVIG is an established treatment in several autoimmune and inflammatory diseases and has been tested in several RCTs in recurrent miscarriage (RM) patients. Although clinically different disorders, RIF has been suggested to share many characteristics with early RM. Immunological parameters that seem associated with both RIF and RM are increased numbers of peripheral blood natural killer cells. There were several reviews of IVIG efficacy in RM patients with high NK cell, but there were few studies in RIF patients.
DESIGN
This retrospective study included 295 cases third IVF cycles between January 2011 and October 2015.
MATERIALS AND METHODS
In 295 cases with previous two IVF-ET failure cycles, 81 women had blood tests for NK cell assay and were treated with intravenous immunoglobulin (IVIG) 400mg/kg on ET day and repeated if pregnancy test was positive (IVIG group). We divided IVIG group into two groups with high NK cell (≥12%) group and normal NK cell (<12%) group.
RESULTS
Total pregnancy rate of third IVF cycle was 29.8% (88/295). In 81 cases, patients had blood tests for NK cell assay and were treated with intravenous immunoglobulin (IVIG group). Among IVIG group, patients with high NK cell (≥12%) were 58.0% (47/81) and normal NK cell (<12%) were 42.0% (34/81). Pregnancy rate was significantly higher in high NK cell group than in normal NK cell group [55.3% (26/47) vs. 26.5% (9/34), p=0.018]. And pregnancy rate was significantly higher in IVIG group with high NK cell than in no IVIG treatment patients [55.3% (26/47) vs. 24.8% (53/214), p=0.015]. But pregnancy rate showed no significant difference between normal NK cell IVIG group and no IVIG treatment patients [26.5% (9/34) vs. 24.8% (53/214), p=0.926]. IVIG treated patients with high NK cell showed improved IVF outcome than patients without IVIG treatment. But IVIG treatment with normal NK cell did not affect IVF outcome.
CONCLUSIONS
IVIG treatment enhances pregnancy rate in RIF patients with high NK cell, but do not affect IVF outcome in patients with normal NK cell. Our results showed that more than half of RIF patients had increased NK cell level. In these patients, IVIG treatment was resulted in increasing more than twice pregnancy rate. Therefore if clinicians encounter repeated IVF failure, we recommend proper evaluation and treatment about RIF causes including NK cell.
-
 2017년 유럽불임학회(ESHRE) P-
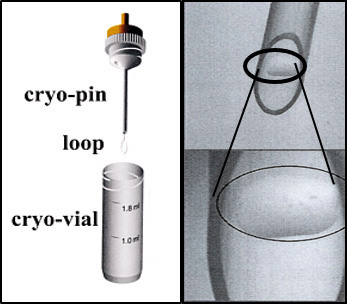
Cryo-loop와 Hemi-straw를 이용한 인간 배아 유리화 동결에서 해동 후 손상되지 않은 배아와 임상 결과의 비교.
2017년 유럽불임학회(ESHRE) P-
Cryo-loop와 Hemi-straw를 이용한 인간 배아 유리화 동결에서 해동 후 손상되지 않은 배아와 임상 결과의 비교.
-
 2016년 미국불임학회(ASRM) P-595
반복착상 실패 환자 에서 면역치료요법이 유용할 것인가; 특히 높은 자연살해세포를 가진 환자에서?
2016년 미국불임학회(ASRM) P-595
반복착상 실패 환자 에서 면역치료요법이 유용할 것인가; 특히 높은 자연살해세포를 가진 환자에서?
-
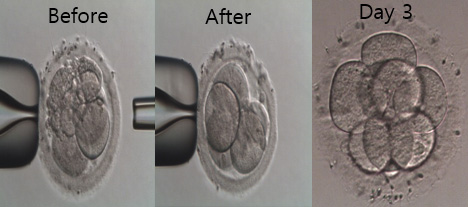 2016년 미국불임학회(ASRM) P-555
2일 째 파편화된 인간 배아에서 파편제거는 순차적 배아의 발달과 임상적 결과를 유의하게 증가시킨다.
2016년 미국불임학회(ASRM) P-555
2일 째 파편화된 인간 배아에서 파편제거는 순차적 배아의 발달과 임상적 결과를 유의하게 증가시킨다.
-
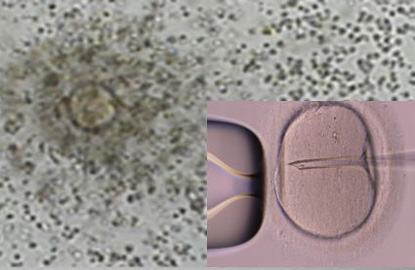 2016년 미국불임학회(ASRM) P-317
정자 DNA 파편화 지수가 높은 환자에서 ICSI가 전통적인 IVF에 비해 임신율을 유의하게 증가시켰다.
2016년 미국불임학회(ASRM) P-317
정자 DNA 파편화 지수가 높은 환자에서 ICSI가 전통적인 IVF에 비해 임신율을 유의하게 증가시켰다.
-
 2016년 미국불임학회(ASRM) P-263
연속 배아 채점 시스템은 Time-lapse 모니터링 시스템 대신 사용할 수 있습니다.
2016년 미국불임학회(ASRM) P-263
연속 배아 채점 시스템은 Time-lapse 모니터링 시스템 대신 사용할 수 있습니다.
-
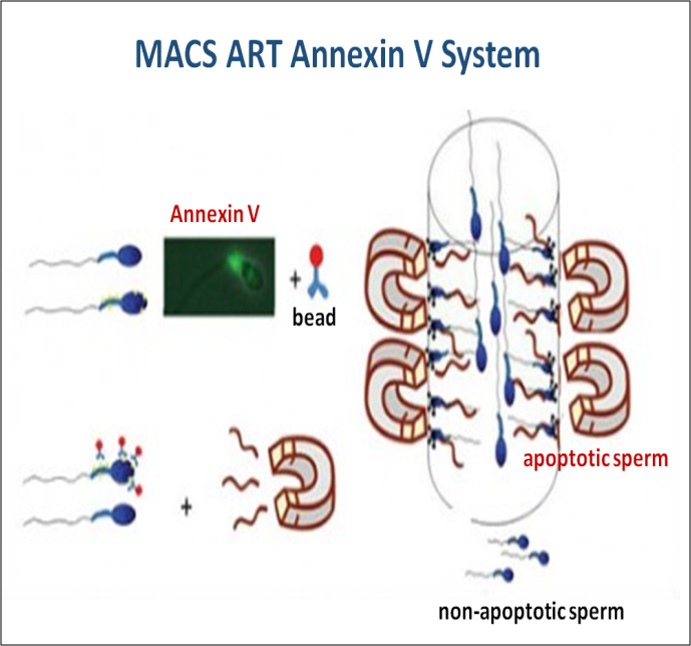 2016년 유럽불임학회(ESHRE) P-021
중층원심분리와 자석활성화세포분리 방법의 병용은 정액샘플의 정자 DNA손상지수를 유의하게 감소시킨다.
2016년 유럽불임학회(ESHRE) P-021
중층원심분리와 자석활성화세포분리 방법의 병용은 정액샘플의 정자 DNA손상지수를 유의하게 감소시킨다.
-
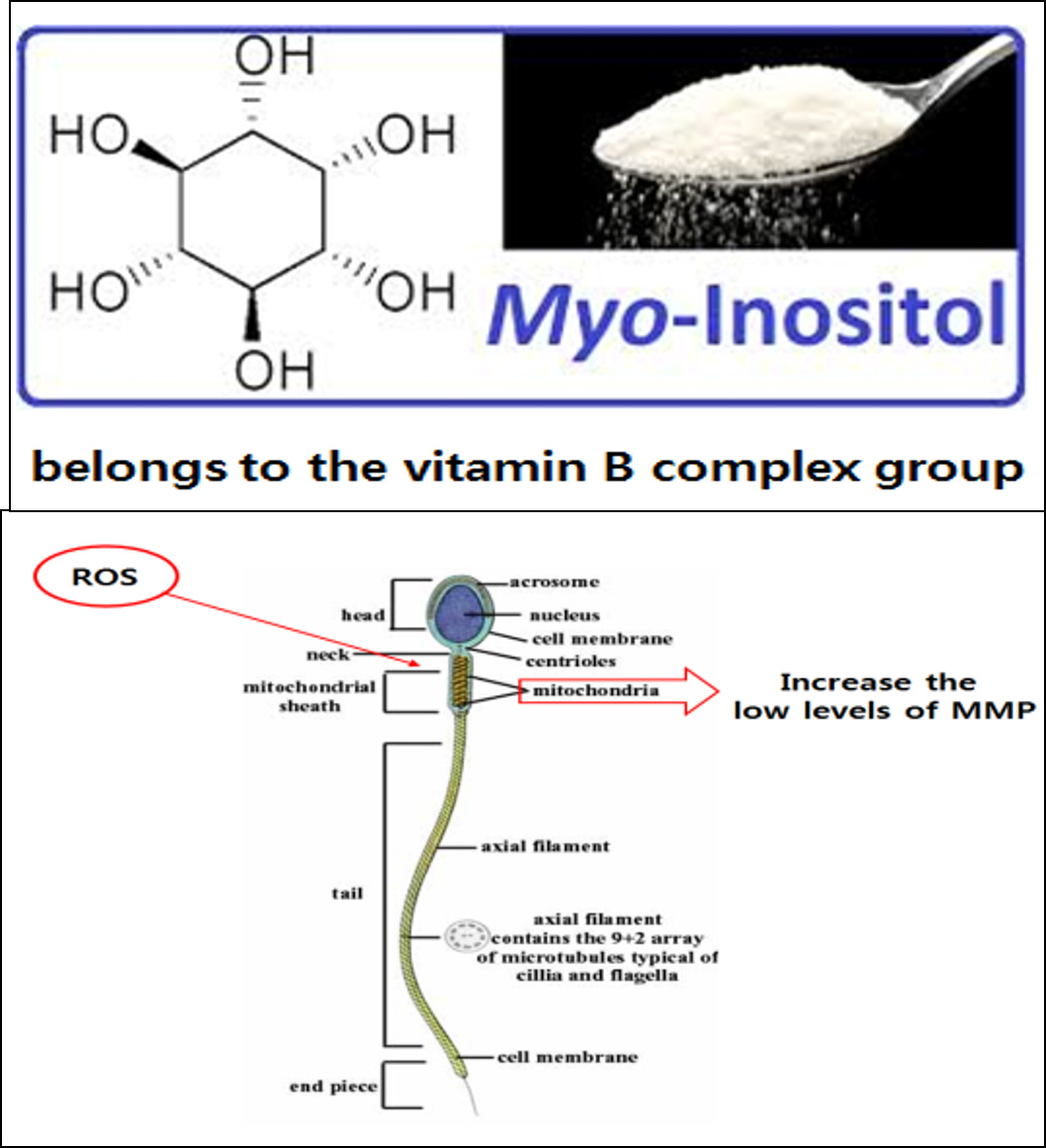 2016년 유럽불임학회(ESHRE) P-022
정액처리 배양액에 Myoinositol의 첨가는 무력정자증 환자의 인공수정시술 시 정자의 운동성과 임신율을 향상시켰다.
2016년 유럽불임학회(ESHRE) P-022
정액처리 배양액에 Myoinositol의 첨가는 무력정자증 환자의 인공수정시술 시 정자의 운동성과 임신율을 향상시켰다.
-
 2016년 유럽불임학회(ESHRE) P-182
다낭성난소증후군 환자의 동결융해배아 이식을 위한 효율적이고 환자친화적인 자궁내막 준비방법; letrozole을 이용한 배란유도
2016년 유럽불임학회(ESHRE) P-182
다낭성난소증후군 환자의 동결융해배아 이식을 위한 효율적이고 환자친화적인 자궁내막 준비방법; letrozole을 이용한 배란유도
울산광역시 남구 삼산로 247 마마파파앤베이비 빌딩 15F - 17F
TEL 052-258-6006 / FAX 052-258-6026
Copyright © mamapapa&baby All Rights Reserved.