홈 > 연구소 > 논문 / 학술활동
연구소
마마파파&베이비의 핵심인 베이비 드림 난임 연구소는
그간의 연구학술 성과에 안주하지 않고,
늘 한계를 뛰어넘기 위해 노력합니다.
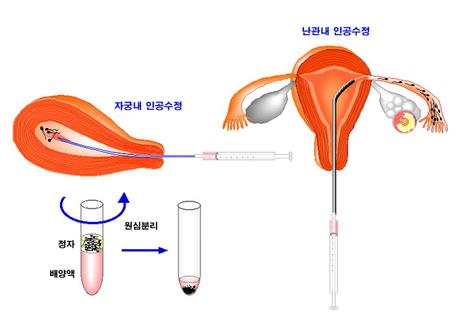
과배란 인공수정 실패 시 다음 인공수정 시술까지 회복기간은 얼마나 필요한가?
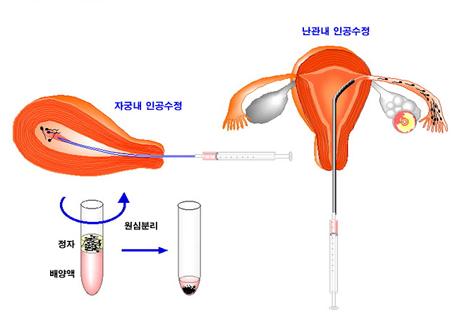
2012년 미국불임학회 (ASRM) P-536 How many months are required for recovery after CC+hMG/IUI failure? (과배란 인공수정 실패 시 다음 인공수정 시술까지 회복기간은 얼마나 필요한가?)
Hong-Gil Sun1, K.H. Lee1, I.H. Park1, S.G. Kim1, J.H. Lee1 and Gyun-Ho Jeon2.
1 Mamapapa&baby OB&GY, 1367-5 Hwashin building 4th floor Dal-dong, Nam-gu Ulsan, X, Republic of Korea, 680-805
2 OBGY, Inje University, Haeundae Paik Hospital, Haeundaero 875, Haeundae-gu Busan, X, Republic of Korea, 612-030.
OBJECTIVE
Controlled ovarian hyperstimulation(COH) can alters endometrial development and impair endometrial receptivity. These changes may affect pregnancy rate in next IUI cycle. In general, it is known that more than two menstrual cycles are needed for recovery after COH. But it is not known adequate recovery period in CC+hMG/IUI cycle. The aim of this study is to evaluate whether recovery period after CC+hMG/IUI failure may affect pregnancy rate in next cycle.
DESIGN
A retrospective study
MATERIALS AND METHODS
The study included 801 patients from January 2010 to October 2011. Clomiphene citrate (100mg/day) was given to patients on days 3-7. Patients were treated with hMG 150 IU on day 8, 10. When the sufficient follicular size and endometrial thickness had been reached, hCG was administrated and insemination was performed. We divided the patients of pregnancy failure into three groups. In group A, inseminations were performed in the following menstrual cycle (385 patients), in group B, after one resting menstrual cycle (119 patients), in group C, after two or more resting menstrual cycles (118 patients).
RESULTS
The study population consisted of 801 patients with average age of 33.5±3.3. We excluded 150 women with successful pregnancy in first attempt (pregnancy rate : 22.60%, 150/801) and 29 women with follow-up loss. Pregnancy rates were 11.17% (43/385) in group A, 10.08% (12/119) in group B and 22.03% (26/118) in group C. Group C and first attempt had significantly higher pregnancy rate than group A and B (P<0.05). Pregnancy rate in group C was similar to that of first attempt insemination (22.03% vs. 22.60%).
CONCLUSION
In cases of none or one resting cycle after failure in CC+hMG/IUI, decreased pregnancy rate was observed probably due to impaired endometrial receptivity. Two or more resting menstrual cycles made similar pregnancy rate to first attempt. In CC+hMG/IUI cycle, we conclude that recovery period may enhance pregnancy rate and a preferred duration is suggested to two or more menstrual cycles.
-
 2012년 미국불임학회 (ASRM) P-264
황체기 보강에서 GnRH 효능제가 나이에 따라 어떤 좋은 이점을 보이는가?
2012년 미국불임학회 (ASRM) P-264
황체기 보강에서 GnRH 효능제가 나이에 따라 어떤 좋은 이점을 보이는가?
-
 2012년 미국불임학회 (ASRM) P-414
시험관 시술의 임신율과 직업과 규칙적인 운동이 어떤 영향을 주게 되는가?
2012년 미국불임학회 (ASRM) P-414
시험관 시술의 임신율과 직업과 규칙적인 운동이 어떤 영향을 주게 되는가?
-
 2012년 미국불임학회 (ASRM) P-536
과배란 인공수정 실패 시 다음 인공수정 시술까지 회복기간은 얼마나 필요한가?
2012년 미국불임학회 (ASRM) P-536
과배란 인공수정 실패 시 다음 인공수정 시술까지 회복기간은 얼마나 필요한가?
-
 2012년 미국불임학회 (ASRM) P-381
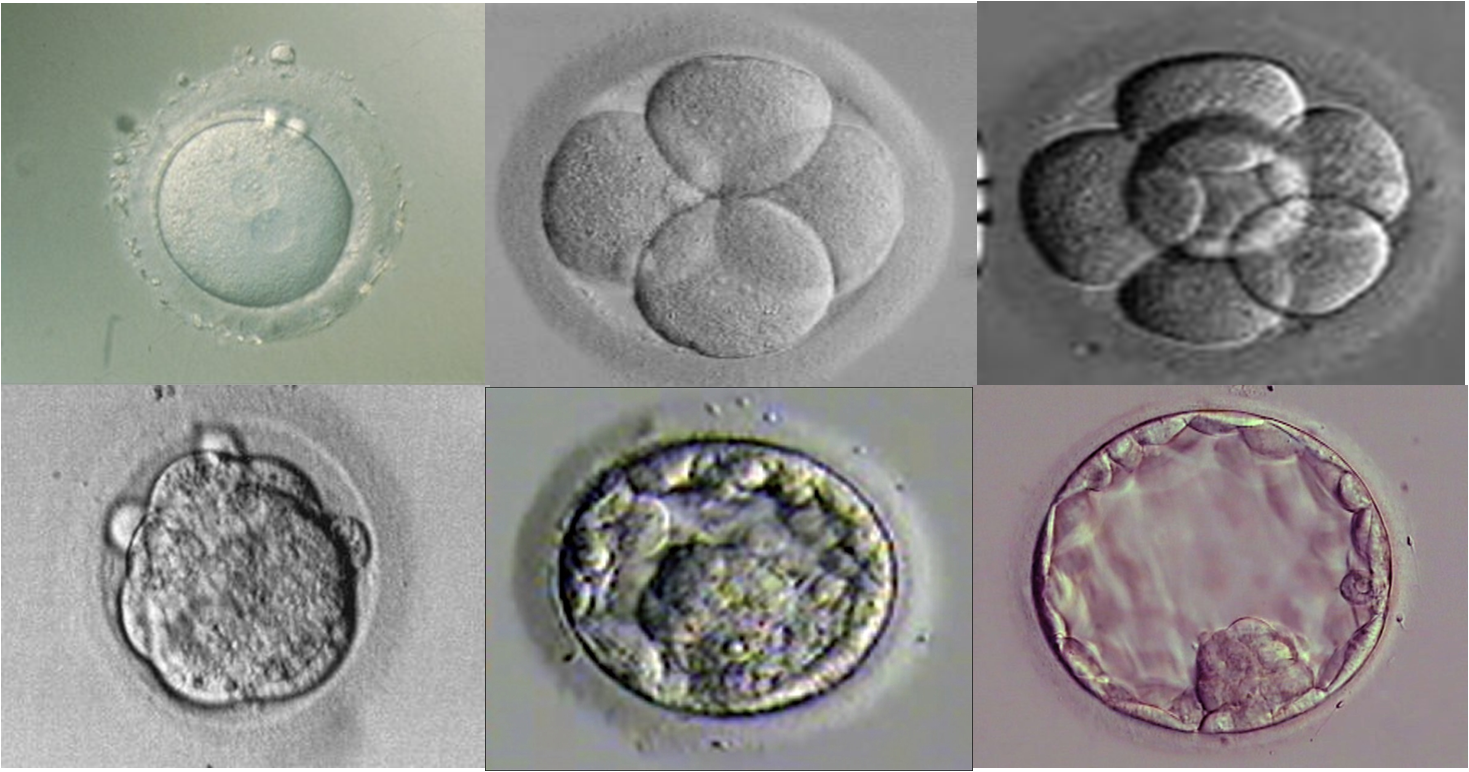
늦게 분열하는 수정란인 경우 동결배아 이식 주기가 보다 좋은 임신율을 보인다.
2012년 미국불임학회 (ASRM) P-381
늦게 분열하는 수정란인 경우 동결배아 이식 주기가 보다 좋은 임신율을 보인다.
-
 2011년 미국불임학회(ASRM) P-510
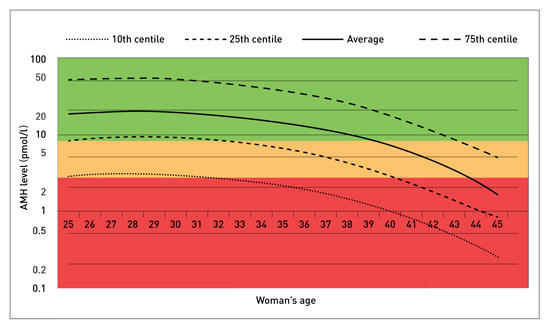
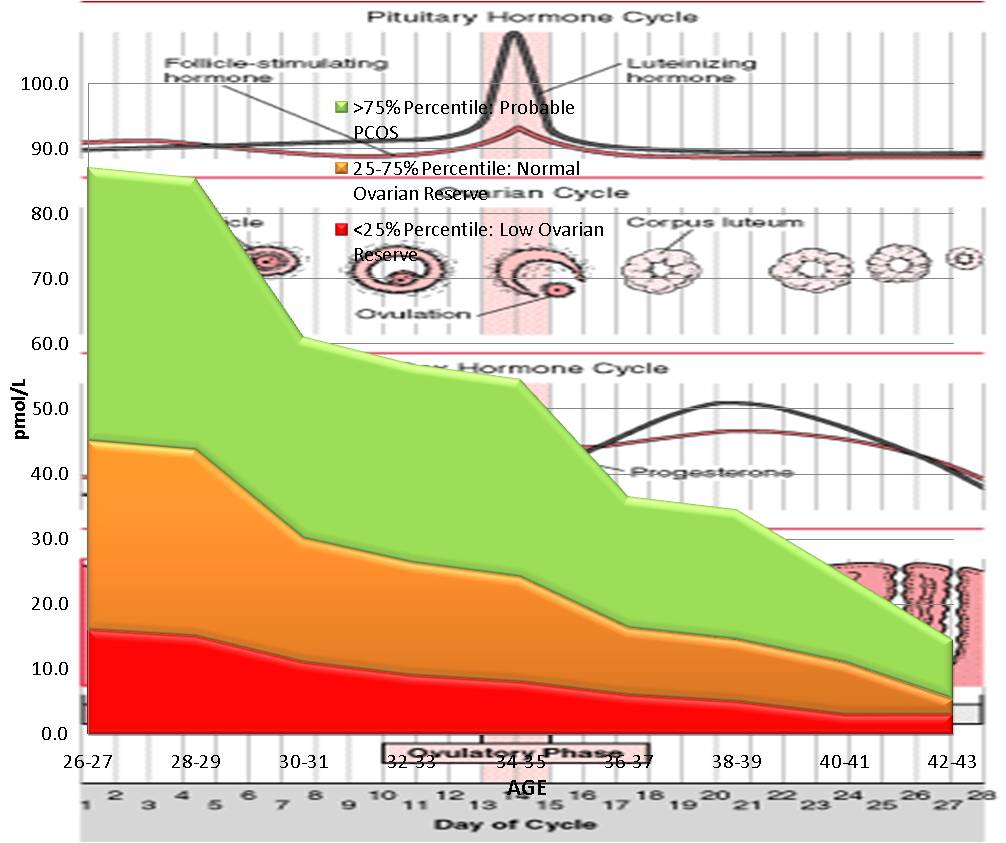
높은 AMH 수치를 보이는 경우 GnRH 효능제 요법이 길항제 요법보다 임신 성공율이 높다.
2011년 미국불임학회(ASRM) P-510
높은 AMH 수치를 보이는 경우 GnRH 효능제 요법이 길항제 요법보다 임신 성공율이 높다.
-
 2011년 미국불임학회(ASRM) P-283
시험관 시술의 결과를 예측하는데 AMH와 생리 3일째의 FSH/LH 비율이 높은 정확도를 가진다.
2011년 미국불임학회(ASRM) P-283
시험관 시술의 결과를 예측하는데 AMH와 생리 3일째의 FSH/LH 비율이 높은 정확도를 가진다.
-
 2011년 유럽불임학회 (ESHRE)P-241
인공수정 시술에서 자궁내막의 두께와 임신율과의 상관 관계
2011년 유럽불임학회 (ESHRE)P-241
인공수정 시술에서 자궁내막의 두께와 임신율과의 상관 관계
-
 2010년 유럽불임학회(ESHRE) P-046
인공수정 시술에서 처리된 정자를 오랜기간 배양하는 것이 임신율에 영향을 주지 않는다.
2010년 유럽불임학회(ESHRE) P-046
인공수정 시술에서 처리된 정자를 오랜기간 배양하는 것이 임신율에 영향을 주지 않는다.
울산광역시 남구 삼산로 247 마마파파앤베이비 빌딩 15F - 17F
TEL 052-258-6006 / FAX 052-258-6026
Copyright © mamapapa&baby All Rights Reserved.