홈 > 연구소 > 논문 / 학술활동
연구소
마마파파&베이비의 핵심인 베이비 드림 난임 연구소는
그간의 연구학술 성과에 안주하지 않고,
늘 한계를 뛰어넘기 위해 노력합니다.
황체기 보강에서 GnRH 효능제가 나이에 따라 어떤 좋은 이점을 보이는가?
2012년 미국불임학회 (ASRM) P-264 Beneficial effects of GnRH agonist in luteal phase: Age-dependent difference. (황체기 보강에서 GnRH 효능제가 나이에 따라 어떤 좋은 이점을 보이는가?)
Il Hae Park, M.D.1, K.H. Lee1, H.G. Sun1, S.G. Kim1, Y.Y. Kim1 and Gyun-Ho Jeon2.
1 Mamapapa & baby OB&GY, 1367-5 Hwashin building 4th floor Dal-dong, Nam-gu Ulsan, X, Republic of Korea, 680-805
2 OBGY, Inje University, Haeundae Paik Hospital, Haeundaero 875, Haeundae-Gu Busan, X, Republic of Korea, 612-030.
OBJECTIVE
Several schemes of luteal phase support (LPS) have been used to increase the chance of pregnancy in controlled ovarian hyperstimulation (COH) IVF cycles. Administration of GnRH agonist has been recently suggested as an alternative for LPS. The purpose of this study is to assess the effects of GnRH agonist addition as a luteal phase support protocol in different age groups.
DESIGN
A retrospective study
MATERIALS AND METHODS
We retrospectively reviewed 489 patients undergoing IVF from April 2011 to February 2012. Women received routine luteal phase support (progesterone only) or GnRH agonist(a single 0.5mg dose of leuporide 6 days after oocyte aspiration) in addition to progesterone. Two groups of patients were formed based on LPS protocols. Group I (conventional LPS group) consisted of patients who received only progesterone. Group II (GnRH agonist addition group) consisted of patients who received progesterone and GnRH agonist. IVF outcomes of two groups were compared in young-age (<35 years) patients and old-age (≥ 35 years) patients.
RESULTS
Age, the number of oocytes, 2PNs, transferred embryos weresimilar between two groups. Pregnancy rate of Group II showed a tendency to increase than that of Group I, but did not show statistical significance [48.9%(111/227) vs. 44.3%(116/262), P=0.07]. In young-age patients (age < 35 years old), Group II had similar pregnancy rates with Group I [58.3%(67/115) vs. 57.1%(84/147), P=0.25]. In old-age patients (age≥ 35 years), Group II had significantly higher pregnancy rates than group I [39.3%(44/112) vs. 27.8%(32/115), P=0.028].
CONCLUSION
Administration of single-dose GnRH agonist in addition to standard luteal support seems to be more effective in old age patients than young age patients. It is probably because luteal phase defect is more common in women as they get older. In this reason, many clinicians give more intensive LPS to old age patients. Therefore, GnRH agonist addition could be a good alternative in old age patients who need more secure LPS.
-
 2012년 미국불임학회 (ASRM) P-264
황체기 보강에서 GnRH 효능제가 나이에 따라 어떤 좋은 이점을 보이는가?
2012년 미국불임학회 (ASRM) P-264
황체기 보강에서 GnRH 효능제가 나이에 따라 어떤 좋은 이점을 보이는가?
-
 2012년 미국불임학회 (ASRM) P-414
시험관 시술의 임신율과 직업과 규칙적인 운동이 어떤 영향을 주게 되는가?
2012년 미국불임학회 (ASRM) P-414
시험관 시술의 임신율과 직업과 규칙적인 운동이 어떤 영향을 주게 되는가?
-
 2012년 미국불임학회 (ASRM) P-536
과배란 인공수정 실패 시 다음 인공수정 시술까지 회복기간은 얼마나 필요한가?
2012년 미국불임학회 (ASRM) P-536
과배란 인공수정 실패 시 다음 인공수정 시술까지 회복기간은 얼마나 필요한가?
-
 2012년 미국불임학회 (ASRM) P-381
늦게 분열하는 수정란인 경우 동결배아 이식 주기가 보다 좋은 임신율을 보인다.
2012년 미국불임학회 (ASRM) P-381
늦게 분열하는 수정란인 경우 동결배아 이식 주기가 보다 좋은 임신율을 보인다.
-
 2011년 미국불임학회(ASRM) P-510
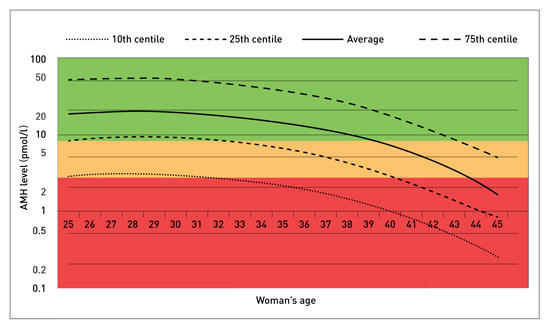
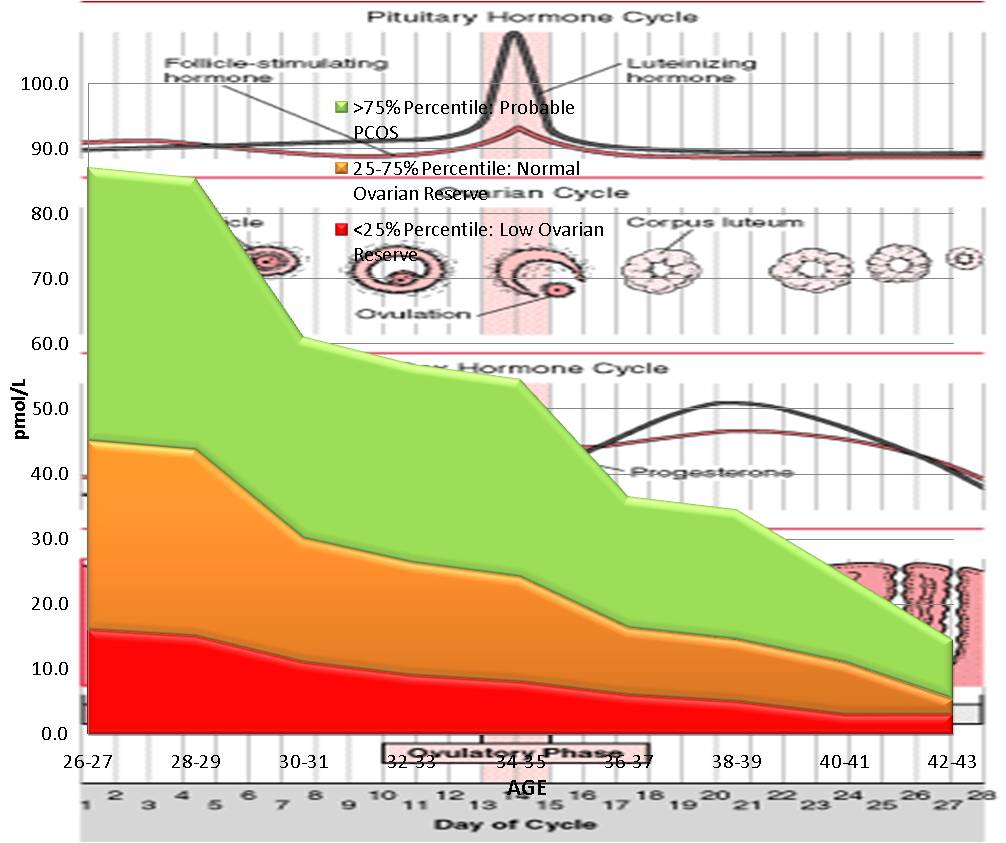
높은 AMH 수치를 보이는 경우 GnRH 효능제 요법이 길항제 요법보다 임신 성공율이 높다.
2011년 미국불임학회(ASRM) P-510
높은 AMH 수치를 보이는 경우 GnRH 효능제 요법이 길항제 요법보다 임신 성공율이 높다.
-
 2011년 미국불임학회(ASRM) P-283
시험관 시술의 결과를 예측하는데 AMH와 생리 3일째의 FSH/LH 비율이 높은 정확도를 가진다.
2011년 미국불임학회(ASRM) P-283
시험관 시술의 결과를 예측하는데 AMH와 생리 3일째의 FSH/LH 비율이 높은 정확도를 가진다.
-
 2011년 유럽불임학회 (ESHRE)P-241
인공수정 시술에서 자궁내막의 두께와 임신율과의 상관 관계
2011년 유럽불임학회 (ESHRE)P-241
인공수정 시술에서 자궁내막의 두께와 임신율과의 상관 관계
-
 2010년 유럽불임학회(ESHRE) P-046
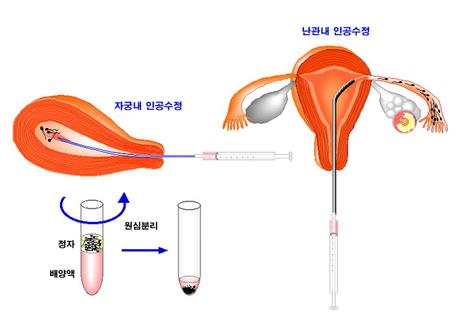
인공수정 시술에서 처리된 정자를 오랜기간 배양하는 것이 임신율에 영향을 주지 않는다.
2010년 유럽불임학회(ESHRE) P-046
인공수정 시술에서 처리된 정자를 오랜기간 배양하는 것이 임신율에 영향을 주지 않는다.
울산광역시 남구 삼산로 247 마마파파앤베이비 빌딩 15F - 17F
TEL 052-258-6006 / FAX 052-258-6026
Copyright © mamapapa&baby All Rights Reserved.